Your diet and health and any medication taken during pregnancy can influence your baby's general health and his teeth. See your dentist to ensure optimal oral health during pregnancy: Infection in your mouth or your teeth can affect your baby and untreated caries in your mouth can increase your baby's susceptibility to tooth decay. Once your child is born, maintain good oral hygiene and try to limit utensil, toothbrush and food sharing to avoid transmitting decay-causing bacteria to your baby.
The first tooth can come in as early as 4 months and as late as 12 months. Children may have some symptoms (irritability, drooling, and/or loss of appetite) but it should not make them sick or cause a fever. If he/she develops a fever, check with your doctor. If he/she has some discomfort, avoid using teething gels. Instead, many babies like a clean teething ring, cool spoon or cold wet washcloth while others simply like the rubbing of their parents' clean finger. Do not give him/her teething biscuits since most of them contain sugars. Don't forget to wipe or brush his/her teeth as soon as they come in!
As for permanent teeth, children rarely have any symptoms when they start coming in except maybe a little sensitivity, especially when chewing.
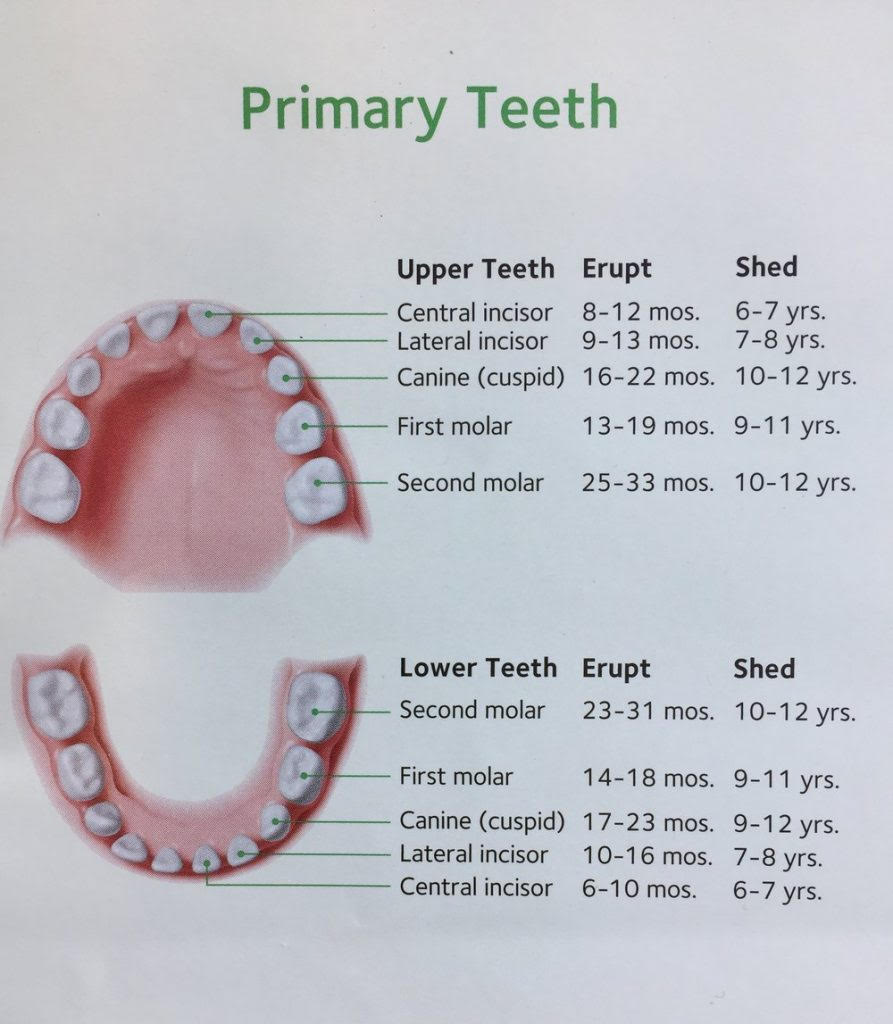
There is a lot of variability in children for the timing of eruption of different teeth. The diagram below is a good indication of the timing of eruption of primary and permanent teeth.
Cavities are caused when sugars in the food we eat and the bacteria in our mouths mix together and produce an acid that eats away at the hard, outer layer of your teeth. If this process happens repetitively, a small hole will form. Different factors will affect at what rate the hole increases in size. Once the hole touches the inner layer of the tooth, the dentin, and can then progress vary rapidly, especially in children.
Cavities are a preventable disease. There are many steps you can take at home to help your child stay cavity free. It is also important to visit the dentist regularly so we can assess your child's condition, help develop a personalized prevention program and if decay does develop, restore it in a conservative way.
The following steps will help your child be part of the cavity-free generation:
The next sections will give you valuable information to help prevent decay for your child.
Regular, thorough brushing is a very important step in preventing tooth decay and gum disease. Brushing removes the bacteria that promote tooth decay and the plaque that can cause gum disease. Ideally, you should brush your child's teeth after every meal because the bacterial attack on teeth begins minutes after eating. You should brush your child's teeth at least twice a day. After brushing your child's teeth at night, make sure he/she does not drink or eat anything (except water). Remember that most children under 8 years old do not have the dexterity to brush their teeth effectively. You must help them brush every night! If you find it difficult to brush your child's teeth, we can demonstrate different techniques during your dental visit.
Flossing removes plaque and bacteria between your teeth that you cannot reach with your toothbrush. If you don't floss your child's teeth, you might be missing more than one-third of his/her tooth surface. You should floss his/her teeth at night just before brushing. We can review with you the best time to start flossing your child's teeth and teach you appropriate techniques.
To maintain a good general and dental health, it is important for your child to have a balanced diet. To help prevent dental caries, it is important to limit the servings of sugars and starches. Since a lot of children prefer these foods, it is important for parents to shop smart: Do not routinely stock your pantry with sugary or starchy snacks. If these foods are not available in your home, it is easier for you and your child to choose better… Make sure he/she does not snack too often and only offer healthy snacks like vegetables and dip, cheese and nuts. If your child likes to chew gum, make sure it is sugarless. Always remember: Water is the beverage of choice between meals.
Fluoride can be found in different sources: water, toothpaste, gels, rinses, tablets and varnish. It is important to have an adequate dose of fluoride to keep our teeth strong. Unfortunately, an excessive dose of fluoride can do harm. Every child has different fluoride needs and we can help determine at his next visit.
Fluoridated toothpaste should be introduced when a child is 2-3 years of age. Make sure the child uses no more than a pea-sized amount on the brush It is important for all older children to use fluoridated toothpaste twice a day when brushing.
In the region of Ottawa, tap water is fluoridated. This can also provide fluoride protection. If you drink well water or live in a region where the water is non fluoridated, it might be preferable for your child to take a fluoride supplement (drops or tablets) but this must be assessed by a dentist.
If your child is at higher risk for decay, other sources of fluoride can be suggested as part of his/her prevention program.
For additional cavity protection, your child might benefit from sealants. Sometimes the tiny grooves and bits on the chewing surfaces of the back teeth are very difficult to clean. A sealant can be applied on those surfaces and will fill all those crevasses preventing food and plaque from being caught there. It resembles a white plastic coating on the teeth and its application is fast and comfortable.
Dental problems can begin early. It is important for your child to have good habits from the start to prevent dental disease. Your child should visit a pediatric dentist when the first tooth comes in, usually between six and twelve months of age. During this visit, your pediatric dentist will help identify any signs of oral disease and develop an oral health care program based on your child's individual needs. Early examination and preventive care will protect your child's smile now and in the future.
A big concern is nursing or baby bottle tooth decay. Your child risks severe decay when he or she nurses continuously from the breast or from a bottle of milk, formula, or juice during naps or at night. Although we encourage breastfeeding, at-will nighttime breast-feeding should be avoided after the first primary (baby) teeth begins to erupt. He/his. Gender neutral. If your child has a tooth, they should never fall asleep with their bottle (unless it contains only water) and their teeth should be wiped after their last bottle before sleeping. Drinking juice from a bottle should always be avoided. To ensure good dental health, infants should be weaned from a bottle or nursing at one year of age. Don't hesitate to ask your pediatric dentist advice on how to make this transition. If your child uses a training/sippy cup between meals, make sure to only fill it with water. Children with caries on their baby teeth are at greater risk of having caries on their permanent teeth. When you brush your child's teeth, look attentively: dull white spots, lines on the teeth next to the gum or dark teeth could be a sign of decay. It is essential to treat decay when present since this could lead to pain and infection for your child.
The sooner you start, the better! Starting at birth (even before your baby has any teeth), clean his/her gums with a clean damp washcloth. Once his/her teeth start to erupt, make sure to clean them well with a cloth or a toothbrush. Brushing with a toothbrush should be started once the teeth erupt. Brush your child's teeth with a small soft-bristled toothbrush and fluoride toothpaste if your pediatric dentist advises it. You should brush your child's teeth at least twice a day. After brushing your baby's or child's teeth at night, make sure he/she does not drink or eat anything (except water). Remember that most children under 8 years old do not have the dexterity to brush their teeth effectively. You must help them brush every night! Most infants do not require flossing but children as early as two years old may greatly benefit from using floss. The use of floss is not age dependent but rather depends on the position of their teeth. We can evaluate if flossing is necessary for your young child and advise you on how to do it as well as teach you age-appropriate brushing techniques.
Your pediatric dentist can review your child's diet and give personalized age appropriate recommendations. Make sure he/she does not snack too often and only offer healthy snacks like vegetables and dip, cheese and nuts. Always remember: Water is the beverage of choice between meals.
This is a form of orthodontic therapy also called phase 1 which attempts to intercept developing problems before they become more severe and harder to correct in the permanent dentition. There are times that children exhibit signs of teeth crowding or jaw problems as they are growing. Children between ages of 6 to 10 years are excellent candidates for early orthodontic care because it takes advantage of the patient’s physical growth potential at a stage when they are growing at a rapid rate. The primary goal of the first phase is to develop a solid foundation for the teeth. Periodic recall appointments are set in order to check the progression of jaw growth and permanent tooth eruption. For this purpose, appliances can be utilized to direct the growth of the jaws and improve teeth alignment.
In summary, early treatment can reduce the cost, duration and complexity of comprehensive orthodontic treatment.
Early or interceptive orthodontic treatment offers several potential benefits outlined below:
Often, at the end of the first phase, the teeth are not in their final position. This will be accomplished during the second-phase. The treatment begins when all the permanent teeth have erupted and consists of straight-forward orthodontic therapy (i.e., braces on all teeth) that will accomplish the final alignment of the teeth. Some patients may even not need to go through this second phase if the main problem was resolved in the first phase.
The major advantage of two-phase therapy is to maximize the opportunity to guide jaw growth and tooth eruption. Optimizing the treatment with the correct timing of the child growth and development is of utmost importance in these cases.
In summary, instead of one comprehensive course of treatment as a teenager, the idea of two phase treatment is to allow the young, growing, child to have some problems solved early and prevent them from suffering with these problems through the years waiting on teeth to erupt and the face to grow. The typical age when full treatment is started is age eleven to thirteen. With phase one treatment, problems are treated between age seven and ten, so the child and the parents do not have to wait until the usual age of orthodontic treatment.
There is no best answer to this question because each orthodontic problem determines its own best starting time in terms of improvement that can be achieved with the least time and expense.
Ages 3 through 6
This age of development includes the children in the primary dentition "baby teeth", or until the eruption of the permanent incisors (front teeth) and first permanent molars. At this young age, severity of the problem will dictate the necessary treatment.
In general, the treatment during this age period is kept simple, since the child has a limited understanding of the problem and limited ability to comply with treatment.
Ages 6 through 12
This age of development following the eruption of the permanent incisors (front teeth) and first permanent molars (six year molars), is commonly referred to as the "mixed dentition stage". This age represents an excellent time for the correction of dental and skeletal problems because:
Problems that are commonly treated during this stage of development include:
Other problems that can be treated during this time period are prolonged thumb and finger sucking habits, abnormal swallowing habits, mouth breathing, excessive tooth crowding.
Treatment planning for these individuals usually emphasizes correction of either skeletal problems (orthopedics), dental problems or both. Custom made appliances are designed according to the problem being treated. They may be removable or fixed. Treatment modalities during this stage of development strive to correctly align the teeth and jaws so that the remaining facial growth will be balanced. Following this early treatment phase, the possibility exists that the patient may never need braces once all his permanent teeth erupt, or if braces are needed during adolescence, the length of treatment is can be shortened.
Every parent wants their child to have a beautiful smile. Early orthodontic treatment can enhance your child’s smile, but the benefits far surpass appearance.
Untreated malocclusions ("bad bites") may contribute to conditions that worsen with age. Crooked and crowded teeth are hard to clean and maintain, which may contribute not only to tooth decay but eventual gum disease. Other orthodontic problems can cause abnormal wear of tooth surfaces, excess stress on the supporting bone and gum tissue, or even misalignment of the jaw joints with resultant chronic headaches or pains in the face and neck.
The importance of an attractive smile should not be under estimated. A pleasing appearance is a vital asset to one's self-confidence, and a child's self esteem often improves as treatment brings teeth, lips and face into harmony. In this way, early orthodontic treatment gives the child a sense of control because it provides an opportunity to participate in the improvement of his or her appearance.
Often parents think that nothing can be done before all the permanent teeth erupt. This is a common misconception. The answer is an emphatic NO! The maximum growth spurt of the child is generally before all his permanent teeth erupt. In many cases, this growth spurt can be used to greatly reduce the problem of your child. If we wait until the jaws have finished their growth, the complexity of treatment can be increased.
Encouraging good dental health habits and providing professional dental care at an early age produce benefits that will last your child a lifetime. Remember, your child should begin regular visits to the pediatric dentist at age 1. Periodic visits and follow-up, will allow the maximum opportunity to prevent future problems from developing and to provide corrective treatment at the best age for your child to have the most beautiful and healthiest smile possible.
If your child has special needs, they might also require a specific dental program adapted to their needs. As pediatric dentists, we have two years of advanced training, beyond dental school, in which we have learned to assess and treat those special children. Your child’s health status or medication may affect his/her diet, his/her risk of oral trauma, his/her ability to brush or even his/her susceptibility to cavities and gum disease. When we see your child, we will take a full medical history as well as review the hygiene and diet habits to help prevent dental disease. It is important that your child be seen by a dentist by his/her first birthday
All children benefit from effective brushing and flossing as well as adequate fluoride. If dental hygiene is difficult for you at home, we can help find techniques appropriate for your child. Your child might also have a particular diet; it is important to assess it and evaluate how it affects his/her dental health.
Different children will have different levels of cooperation at the office. Our office is very children friendly, and a lot of children will let us examine them by using a gentle caring approach. If your child would benefit from a dental treatment, we have a comprehensive education in behavior management and after assessing your child needs, it would be our pleasure to explain the possible techniques with you.
Primary or baby teeth are the foundation of the permanent dentition. In other words, they are the key to healthy and well aligned permanent or adult teeth. Their position in the jaw maintains the proper place for the underlying permanent teeth. Primary teeth also help your child speak clearly and chew naturally.
If a primary tooth has a cavity, it is essential that an appropriate treatment be done before it breaks down, becomes infected and/or is lost early, since it can adversely affect the development and health of the permanent teeth. In other words, there is a great chance that the permanent (adult) teeth will not grow in their proper position and this can affect the way your child’s permanent teeth close together (occlusion or bite). Furthermore, your child might suffer a great deal of pain from a dental cavity or even develop a mouth or facial infection which can be very serious for his health. If your child develops pain or infection, it can influence his eating habits, his sleep, his concentration at school and therefore his general well being.
In summary, the preservation of “baby tooth” is far more important than the false myth that "...nothing needs to be done because they are going to fall out sooner or later."
Decay can have many appearances. When you brush your child’s teeth, take a careful look at them. Large decay often presents itself as a cavity (a hole) but smaller decay can appear as either a chalky white, yellow or brown stain. It can be present close to the gum line, on the top surface or anywhere else on the tooth. One of the most common sites for decay on primary teeth is between the teeth. Unfortunately our eyes can not see there and that is why it is often important to take X-rays to make sure we can assess the whole situation. If you suspect that something you see on your child’s teeth might be decay, it is important to let us know so we can see your child as soon as possible. Don’t forget to visit us regularly so we can make a thorough examination of your child’s teeth because decay is not always obvious.
The type of treatment chosen to repair a cavity will depend on your child’s age, his cavity risk, his dental hygiene, as well as the size and position of the cavity. In general, a lot of the procedures are similar to the ones for permanent teeth but adapted to primary teeth.
For anterior teeth, aesthetics is an important concern when we restore the teeth and we can discuss the different options for your child.
As for posterior (back) teeth, the three main types of restorations are amalgam fillings (silver), bonded fillings (white) and stainless steel crowns:
For more information on types of fillings, visit the Canadian Dental Association website:
http://www.cda-adc.ca/english/your_oral_health/dental_procedures/restorative_materials/default.asp#1
If the cavity has spread to the nerve of the tooth, a pulpotomy (partial root canal treatment on a baby tooth) will be necessary to save the tooth. This procedure involves removing part of the nerve tissue and placing special medication on the remaining tissue so it can heal.
If the tooth has developed infection or an abscess, a thorough evaluation of the conditions will be performed and we will discuss if it is preferable to perform a pulpectomy (partial root canal to remove infected nerve tissue of the baby tooth), a full root canal treatment, or a tooth extraction.
When a posterior tooth cannot be saved and must be extracted, a space maintainer might be required to prevent the adjacent tooth from moving into the empty space, keeping the space necessary for the eventual eruption of the corresponding adult tooth. Space maintainers are little appliances, usually made of metal, and are usually very well tolerated by children.
Just like all children are different, they all react differently at the dentist. Many techniques exist to help your child have a good experience at the dentist. We will discuss and choose appropriate techniques for your child depending on his age, the dental procedures required for your child, his past experiences and his health status, and will continually adjust according to his level of cooperation during the examination visit.
We are trained in many methods to help children feel comfortable with dental treatment. We will almost always use a technique called “Tell-Show-Do” which consists in explaining to your child what is to be done, then demonstrating with instruments before the procedure is performed in your child’s mouth. We will also constantly reward desirable behaviors with compliments and praise. The office is also designed such that your child can watch a movie throughout his appointment thereby keeping them distracted during the treatment.
Sometimes, however, if your child is anxious, very young and/or uncooperative, he may need more support than a simple "Tell-Show-Do.” There are different management options available to help your child cope better with dental treatment:
In summary, during your visit, we will be able to discuss with you which behavior management option is the best for your child. We know that all children are not alike and therefore, every treatment is tailored to your child’s best need as an individual.

Indications
To repair small/medium “cavities” in primary (baby) and permanent (adult) teeth.
Also used for broken teeth after a trauma (like a fall)
Advantages
- Strong & Durable if placed in the right circumstances
- White
- conservative
Disadvantages
- Can be followed by tooth sensitivity
- Can have new decay around it
- Requires a very controlled environment to be done correctly
Indications
- Small cavities in primary (baby)teeth
- Temporary filling
- When fluoride release is especially desirable
- Hypoplastic (defective) teeth
Advantages
- Somewhat moisture tolerant
- Fluoride-releasing
- Minimal sensitivity
Disadvantages
- Wears faster than composite
- More prone to fracture

Indications
- Medium/large cavities on primary teeth
- After pulp/nerve treatment
- Teeth with hypoplasia(including adult teeth)
- When failure of other restorative materials is likely
- If there is recurrent decay under a previous white filling
- Small cavities on a child who is high risk of recurrent decay or requires treatment under general anesthesia.
Advantages
- 95% of primary teeth treated with SSC will not require any further treatment prior to the tooth exfoliating (falling out)
- Covers the tooth preventing breakdown and recurrent decay
Disadvantages
- Esthetics (silver colour)
Indications
- Small/medium cavities on a primary tooth.
- Child must be able to tolerate xray of the tooth
- Intended for a child unable to tolerate treatment with local anesthesia (freezing)
Advantages
- No local anesthetic
- No or minimal tooth reduction.
- Quicker than conventional treatment
- Reduces need for sedation
Disadvantages
- Temporary discomfort and pressure with placement
- Occlusion (‘the bite’) will feel off at first.
- May perforate (wear) and require replacement.
- Incomplete cavity removal (risk of cavity progression)
- May require separate visit to place elastic separators; separators may be uncomfortable while worn.

Indications
- Same indications as SSC
- Requires adequate spacing between teeth
- Instead of SSC in a child with a nickel allergy
Advantages
- Esthetics (white)
Disadvantages
- Take longer to place, more difficult
- Require excellent patient behavior, or general anesthesia
- Requires more removal of tooth structure than SSC
- Debond (come off) or fracture more easily than SSC.
- Cost

Indications
- Medium/large cavities on a primary front tooth
- Primary tooth that has had pulp/nerve treatment
- Cavity that extends to the level of the gingiva (gumline)
- Requires adequate spacing between teeth
Advantages
- Esthetics (white)
- Good gingival health
- Durable
Disadvantages
- Technique sensitive
- Require excellent patient behavior, or general anesthesia
- Not easily repaired (easily replaced)
- Can debond/deciment

Indications
- Medium/large cavities on a primary front tooth
- Primary front tooth that has had pulp/nerve treatment
- Trauma of primary tooth
- Small caries in a child at high risk of caries
Advantages
- Esthetics (white)
- Can stain and chip
- Can be repaired
Disadvantages
- Technique sensitive
- Require excellent patient behavior, or general anesthesia

Indications
- Infection or extensive decay of a primary tooth
Advantages
- Removes source of pain/infection
- When a tooth is extracted early a spacer may be recommended to help keep the space open and prevent teeth from shifting until its time for the adult tooth to grow in. The main type of appliance is called a Band and Loop. When the permanent tooth is ready to erupt, we will remove the appliance without any need of sedation.
Disadvantages
- Space maintainers can debond and require recementation.
- The abutment (tooth that holds on the space maintainer) is at higher risk of getting a cavity.


Indications
- Small/medium sized cavities in primary teeth
- Temporary restoration often used to delay conventional treatment in a child unlikely to tolerate local anesthesia (freezing)
Advantages
- Can be done without local anesthesia
- Slows/stops cavity progression and food impaction
Disadvantages
- Will be stained black around the edges of the filling
- Will eventually require replacement or conventional filling or crown or extraction.
- Cavity may still progress and could get worse
Indications
- Deep groove morphology on molar
- Child or teen who is high risk for cavities
Advantages
- Prevents cavities in the pits and fissures of molars
- Longevity, if done in ideal conditions, is best of sealant materials (average 3 years)
Disadvantages
- Technique sensitive
- Requires a clean, dry field and good patient cooperation.
- Minimal/no fluoride release

Indications
- Same as for resin sealant
- Can be done a tooth that is partially erupted or difficult to isolate
- Often recommended for teeth with hypoplasia (enamel defect)
Advantages
- Prevents cavities in the pits and fissures of molars
- Releases fluoride
- Longevity better than resin if conditions are not ideal
Disadvantages
- Requires a clean, dry field but is somewhat moisture tolerant.
- Often pink in colour(but not very visible)
Numbing can last 1-4 hours after the visit and can be very difficult for children. They will often ask to “make it go away”, and may be sad or upset about it. It is uncomfortable and they often refer to it as pain.
While numb: Only eat a liquid diet (yogourt, apple sauce)
Cold foods typically feel better for your child.
There is a high risk of self injury by biting their lip, cheek tongue: Monitor them carefully! If they bite themselves, it may bleed, swell, and look ulcerated and mimic an infection.
A new filling may feel different at first - it may be uncomfortable for 1-2 days. Acetaminophen (Tylenol) and/or Ibuprofen (Advil/Motrin) can be given for pain.
There may be some sensitivity to change in temperature for the first weeks.
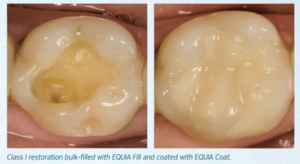
Glass ionomer/fluoride releasing filling: Fluoride releasing sealants (pink or white) and fillings gradually obtain their full strength: Keep a liquid diet for 1 hour and avoid crunchy foods for 24 hours.
Your child should avoid using the front teeth to bite directly into hard foods.
Watch for signs of infection such as pain, increased mobility, swelling or a pimple on the gum tissue above the tooth; if present, contact our office for further evaluation.
Placement of a crown causes a lot of pressure on the gum: the gum around the crown may be sensitive for 1 week and may bleed during brushing. Even if bleeding, continue to keep the area clean with brushing. It often takes a few days to a week for children to adjust to their crown. Monitor them carefully: they should not pick or pull on their crown as this may pull it off.
Acetaminophen (Tylenol) and/or Ibuprofen (Advil/Motrin) can be given for pain.
Sticky foods can pull off a crown and should be avoided/limited.
Because zirconia/white crowns are only cement-retained, they are especially susceptible to coming off.
Foods to avoid: Gum, taffy, caramels, suckers, other sticky or hard candies. Such foods are preferable to be avoided until the tooth naturally falls out.
Placement of a space maintainer causes pressure on the gum and may feel different at first. It may take a few days for your child to adjust to the spacer.
Your child should avoid pulling on or poking the wire.
Keep your child away from sticky, chewy, hard, crunchy foods as listed below. These foods can get wrapped around the wire, bend the wire, get stuck in the band, causing the appliance to break or become loose.
Foods to avoid: Gum, taffy, caramels, suckers, other sticky or hard candies, etc.
If the space maintainer becomes loose or breaks, contact our office so we can evaluate if the appliance needs to be recemented or remade. Expect the spacer to need to be recemented multiple times during its lifespan.
Numbing/Local anesthetic: Please read the “local anesthesia/numbing” section above.
Bleeding – Be sure the pad is folded so that the pressure is directed specifically to the extraction site. Gauze pressure for 10-20min in the area should stop any bleeding. This can be done by biting on the pad or for young children, the parent can hold it in place. Some mild oozing can continue that day. If the bleeding is not stopped within 30-45 minutes, contact the office.
Discomfort – Pain following an extraction can be managed with children’s Tylenol, Advil or Motrin as needed.
Swelling – If swelling should occur, use an ice pack or cold pack on the cheek over the extracted area. Never apply heat over the swollen area.
Activity – Have the patient relax for about 3-4 hours after the extraction appointment. Avoid situations where trauma could be a problem. Avoid swimming pools for at least 24 hours because of bacteria in the water.
Eating/Drinking – Respect the “while numb” diet at first. Once numbing has disappeared: For the first 24 hours: Keep a very soft diet (i.e. scrambled eggs, macaroni and cheese or other bland foods), avoid drinking from a straw or active spitting. Avoid foods that require considerable biting (sandwiches, bagels, etc.) for 48 hours.
Suture – If sutures are placed, they will resorb on their own within 5-7 days. No follow-up appointment is needed, unless you suspect anything unusual.
Hygiene care – One day after extraction(s), your child can gently rinse his/her mouth with lukewarm salt water, especially after meals. This can help keep the extraction area clean and may speed healing. The teeth should be brushed normally except in the area of extraction(s).
At Kids and Teens, we offer three types of sedation to help your child’s appointment go smoothly and
ensure they have a good experience at the dentist.
 It's a colourless and odourless gas that helps the child feel more relaxed and comfortable during their treatment. During treatment they will be awake and will be more focus on the tv then what we're doing. This is the mildest form of sedation and is a good option for kids who have good cooperation during cleanings, visits, and have no fear of the dentist. Before this appointment we ask that the patient fasts for 2 hours prior to their appointment.
It's a colourless and odourless gas that helps the child feel more relaxed and comfortable during their treatment. During treatment they will be awake and will be more focus on the tv then what we're doing. This is the mildest form of sedation and is a good option for kids who have good cooperation during cleanings, visits, and have no fear of the dentist. Before this appointment we ask that the patient fasts for 2 hours prior to their appointment.
 This method of sedation is a liquid medication that is used along aside Nitrous Oxide (laughing gas). This is still classified as a mild form of sedation where the child will be awake and not fully asleep for the treatment. The two types of medication we use at our office is Hydroxyzine and Midazolam. Which type is used will be determined by the dentist. The patient comes in initially to see the nurse to have their vitals taken along with going over their fasting and making sure it's safe to proceed. The child will stay with the nurse up to 1 hour before the dentist sees them for treatment. After the appointment the child cannot go to school as the medication stays in their system for up to 8 hours.
This method of sedation is a liquid medication that is used along aside Nitrous Oxide (laughing gas). This is still classified as a mild form of sedation where the child will be awake and not fully asleep for the treatment. The two types of medication we use at our office is Hydroxyzine and Midazolam. Which type is used will be determined by the dentist. The patient comes in initially to see the nurse to have their vitals taken along with going over their fasting and making sure it's safe to proceed. The child will stay with the nurse up to 1 hour before the dentist sees them for treatment. After the appointment the child cannot go to school as the medication stays in their system for up to 8 hours.
 GA is the only form of sedation that can be offered for children where the patient will be fully “a sleep”. This option is performed at a surgical center located on Carling Ave where an anesthesiologist from Cheo, will be the medical doctor present providing care for your child. We require a telephone consult prior to the surgical appointment as we have a lot of information and medical forms to discuss before treatment.
GA is the only form of sedation that can be offered for children where the patient will be fully “a sleep”. This option is performed at a surgical center located on Carling Ave where an anesthesiologist from Cheo, will be the medical doctor present providing care for your child. We require a telephone consult prior to the surgical appointment as we have a lot of information and medical forms to discuss before treatment.